Project
The first European MSM Internet Survey (EMIS-2010) was co-ordinated by Robert Koch Institute (Berlin). It received funding from the European Union, under the framework of the Health Programme, as stipulated in Grant Agreement 2008 12 14 of the Executive Agency for Health and Consumers (EAHC). Further funding was received from CEEISCat (Centre d’Estudis Epidemiologics sobre les ITS/HIV/SIDA de Catalunya, Spain); Department of Health for England; Maastricht University (The Netherlands); Regione del Veneto (Italy); and Robert Koch Institute (Germany). Further funding for the participation of men in specific countries was provided by: German Ministry of Health for Ukraine and Moldova; Finnish Ministry of Health for Finland; Norwegian Institute of Public Health for Norway; Swedish Board of Health and Welfare for Sweden; and Bundeszentrale fur gesundheitliche Aufklarung (BZgA) for Germany.
From 2009, a large network was built to create an online questionnaire to find answers to four research questions. Scientists and activists from community-based NGOs jointly prepared, pre-tested, and ran the survey.
In summer 2010, an online questionnaire was run simultaneously in 25 different languages: Bulgarian (български език), Czech (Čeština), Danish (Dansk), German (Deutsch), Estonian (Eesti keel), Greek (Ελληνικά), English, Spanish (Español), French (Français), Italian (Italiano), Latvian (Latviešu valodam), Lithuanian (Lietuvių kalba), Hungarian (Magyar nyelv), Dutch (Nederlands), Norwegian (Norsk), Polish (Polski), Portuguese (Português), Romanian (Română), Russian (Pусский язык), Slovenian (Slovenščina), Serbian (Srpski), Swedish (Svenska), Finnish (Suomi), Turkish (Türkçe), and Ukrainian (Yкраї́нська мо́ва). Respondents were invited through individual messages from multi-national dating websites, or through banners on (country-specific) websites.
EMIS-2010 was the first study designed to collect self-reported data from MSM across Europe. The data was used as a baseline for follow-up surveys and for cross-sectional analyses – comparing different groups of MSM with different needs, comparing different countries or regions, etc.
EMIS-2010 results informed the planning of prevention interventions for MSM by identifying prevention needs commonly unmet across MSM (priority aims), and sub-groups of MSM for whom many prevention needs are also poorly met (priority target groups).
Historical background
Surveys of sexual behaviour and prevention needs among men who have sex with men (MSM) had been primarily conducted on national levels. Due to different sampling methods (particularly Internet-based vs. venue-based) across countries, and because of similar, but not identical questions, a harmonisation of indicators was needed to allow, among other things, reporting of comparable data to the European Centre for Disease Prevention and Control (ECDC). In the early 2000s, MSM networking and dating website had been shown to be (cost-)effective and valid means for recruiting respondents.
Research questions and covered items
The EMIS-2010 questionnaire was structured by four questions (research priorities):
- What are the levels and distributions of sexual HIV/STI exposure and transmission facilitators?
- What are the levels and distributions of unmet (prevention) needs of MSM?
- What is the population coverage / what are the biases of prevention interventions?
- What information is needed to compare samples and target interventions?
As to research priority number one, the EMIS questionnaire coveed all six core indicators (#1-6) and nine of ten population-specific indicators for MSM (#7-15) suggested by the European Centre for Disease Prevention and Control.
- Numbers of sex partners in the last 12 months
- Use of condom at last (anal) intercourse, separate for steady vs. non-steady partners
- Tested for HIV, ever and in the last 12 months; year and result of the last test
- Having paid for sex in the last 12 months; use of condoms at last paid intercourse
- Level of education (ISCED-1997); nationality/‘origin’, sexual orientation (Kinsey modified classification)
- Knowledge (identify ways of preventing sexual HIV transmission, reject major misconceptions)
- Age at 1st sex
- Recent STIs
- Condom use with different types of partners
- Exposure to risk (last 12 months)
- Recency and result of hepatitis C test
- Types of drugs consumed
- Proportion on treatment
- (Detectable or undetectable) viral load
- CD4 count (at diagnosis)
To balance questions on behavioural surveillance with items needed for prevention planning, including needs for policy and structural interventions, EMIS also included the following question areas needed to cover priorities two and three above:
- Knowledge (transmission, risks, non-risk, safe condom use, PEP)
- Problems related to alcohol and recreational drug use, types of drugs and recency of drug use
- Barriers to early treatment
- Vaccination and circumcision
- HIV-related discrimination
- Anti-gay violence / Homophobia
- Access to gay-specific information
- Access to and experience with condoms
- Access to testing (HIV/STI)
- Used HIV/STI testing sites, service performance regarding MSM
- Relationships
- Loneliness and friendships
- Sexual happiness
- Idea of the best sex life
- The sexiest man on the planet
All 25 EMIS-2010 questionnaires are available for download. Individuals and organisations are welcome to use individual questions, or the whole questionnaire, on the understanding that they credit the EMIS project in any written outputs arising from their use.
Response
EMIS-2010 collected data between June 4 and August 31, 2010.
It was promoted online and offline through media for gay, bisexual, and other men who have sex with men (MSM). Following the slogan “Be part of something huge!”, more than 180,000 MSM living in 38 countries across Europe, and more than 160,000 MSM living in the 27 (at the time) EU member states completed the questionnaire.
EMIS-2010 was thus the largest international study ever conducted on homosexually active men. This overwhelming response to a 20-minute survey demonstrated both a highly acceptable instrument and high community engagement. Neither would have been possible without the participation and support of local, national, and international LGBT organisations, as well as of pan-European gay-organised social online networks like GayRomeo, Manhunt, Qruiser, Qguys, or Gaydar.
The following map shows the number of respondents per 10,000 inhabitants per country.

Sub-regions
One of the objectives of EMIS-2010 was to generate comparable population level data needed for HIV prevention planning across countries. Given that EMIS ultimately covered 38 countries, geographical patterns are difficult to see when looking at tables with 38 rows, or when looking at diagrams with 38 bars. To increase the utility of our graphic presentations, countries were grouped into European sub-regions.
The United Nations provide several different approaches to grouping European sub-regions.
- WHO for example distinguishes three sub-regions within Europe – broadly based on the political history of the second half of the 19th century. Because political structures of countries have an impact on the geographical formation of epidemics, such as the HIV epidemic, this grouping is highly relevant for the analysis of EMIS-2010 data. However, the WHO grouping leaves us with only three geographical entities:
- The WHO sub-region of Eastern Europe includes all succession states of the Soviet Union. This means that some countries in that sub-region today are part of the European Union (such as the three Baltic states), or they are located outside Europe. However EMIS-2010 was not funded to include residents of countries in central Asia or in the Caucasus.
- The WHO sub-region of Central Europe too encompasses a wide range of countries, such as all other (non-Soviet Union) European former Comecon members (or their succession states), as well the succession states of Yugoslavia; Turkey and Cyprus.
The WHO sub-region of Western Europe is broadly identical (except for Malta) to the 15 European Union member states as of 1995, plus EEA/EFTA countries such as Norway and Switzerland.
A typical grouping for EU-funded analyses is the distinction between old (as of 1995) and new (as of 2004/2007) EU member states, and non-EU/EFTA countries. A problem with this grouping, as with the WHO sub-regions, is the large variance in political histories of the countries within each sub-region. Political and societal systems have a substantial influence on how health care is organised, on the social acceptance of sexual behaviours and identities outside the heterosexual norm, or on the permeability of borders, and hence mobility. All these factors can broadly influence the onset and course of infectious disease epidemics, such as infections with HIV or other sexually transmissible pathogens.
EMIS-2010 data covers 18 countries within the WHO sub-region of Western Europe (AT, BE, CH, DE, DK, ES, FI, FR, GR, IE, IT, LU, MT, NL, NO, PT, SE, UK); 13 countries within the WHO sub-region of Central Europe (BA, BG, CY, CZ, HR, HU, MK, PL, RO, RS, SI, SK, TR); and 7 countries within the WHO sub-region of Eastern Europe (BY, EE, LT, LV, MD, RU, UA).
As for the grouping typical for EU-funded analyses, EMIS-2010 data covers the 17 old EU/EFTA countries (as Western Europe above, without Malta); 12 new EU member states (BG, CY, CZ, EE, HU, MT, LT, LV, PL, RO, SI, SK); and 9 non-EU/EFTA member states (BA, BY, HR, MD, MK, RS, RU, TR, UA).
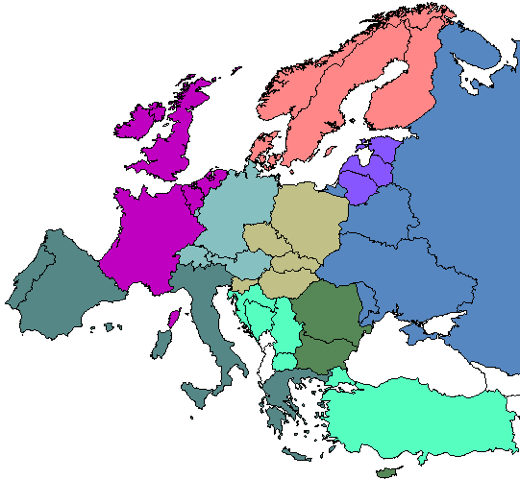
Because these two groupings do not match, and because in many analyses of EMIS-2010 data they would mask important differences, in the 2010 European report we used a third classification with nine sub-regions, each consisting of fewer and more comparable countries. Depending on how these nine sub-regions are combined, both the WHO and the EU groupings described above can be re-constructed. The placement of Greece and Malta in our grouping seems geographically counter-intuitive, but was needed to match the WHO and the EU groupings.
The nine sub-regions of Europe used in EMIS-2010 publications are:
- West – Belgium (BE), France (FR), Ireland (IE), the Netherlands (NL), and the United Kingdom (UK).
- North West – Denmark (DK), Finland (FI), Norway (NO), and Sweden (SE).
- Central-West – Austria (AT), Switzerland (CH), Germany (DE), and Luxembourg (LU).
- South West – Greece (GR), Spain (ES), Italy (IT), and Portugal (PT).
- North East – Estonia (EE), Lithuania (LT), Latvia (LV).
- Central-East – The Czech Republic (CZ), Hungary (HU), Poland (PL), Slovenia (SI), and Slovakia (SK).
- South East (EU, as of 2010) – Bulgaria (BG), Cyprus (CY), Malta (MT), and Romania (RO)
- South East (non-EU, as of 2010) – Bosnia and Herzegovina (BA), Croatia (HR), Macedonia (MK), Serbia (RS), and Turkey (TR).
- East – Belarus (BY), Moldova (MD), Russia (RU), and Ukraine (UA).
The rationale for grouping EMIS-2010 countries the way we did was two-fold. First, we wanted to use names that are intuitive to the reader, and used or suggested by international organisations. Second, we thought it useful to base the grouping of sub-regions on data that is crucial for the purpose of our research.
The United Nations Group of Experts on Geographical Names* suggested 6 European sub-regions: North Europe, West Europe, Central Europe, East Europe, South Europe, and South East Europe. Most ambiguity exists with the definition of Central Europe. Out of a plethora of different definitions, WHO is the only organisation that groups Balkan countries, Southeastern European countries such as Bulgaria or Romania, or Turkey or Cyprus as Central Europe. Therefore, in this report, when using WHO regions, we highlight this by referring to “the WHO sub-region of Central Europe”. The EMIS definition of Central Europe is much narrower, and it includes both countries of the WHO sub-region of Western Europe (Austria, Germany, Luxembourg, Switzerland =Central-West) as well as countries of the WHO sub-region of Central Europe (Poland, the Czech Republic, Slovakia, Hungary, and Slovenia =Central-East).
Greece was grouped with South West Europe, while Malta was grouped with South East Europe. The only reason for this geographically counter-intuitive grouping was that by doing so both the WHO regions and the EU-typical grouping can be reconstructed. For the same reason, we further divided South East Europe into EU and non-EU countries. The Baltic countries were labelled North East, whereas the Scandinavian countries and Finland were labelled North West.
*United Nations Group of Experts on Geographical Names (UNGEGN, 2006) Working Paper Number 48: A Subdivision of Europe into Larger Regions by Cultural Criteria. Twenty-third Session Vienna, 28 March – 4 April 2006